By Kari Radjewski, Director of Marketing & Communications at the Children’s Foundation
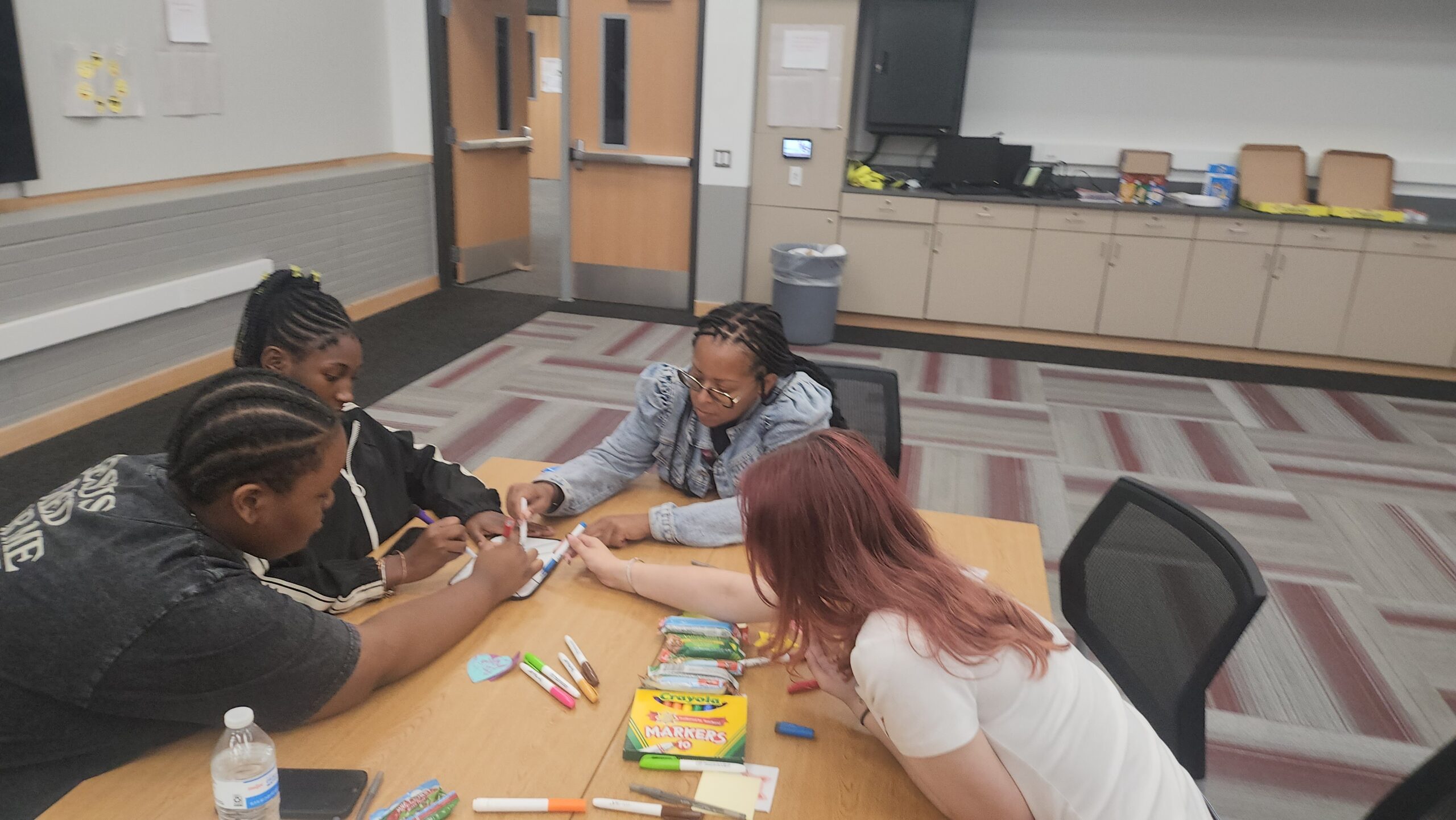
Since opening in late 2022, the Adolescent Addiction Recovery Center, or AARC as many have come to know it, has made its mark on the community. Philanthropically funded by the Jamie Daniels Foundation and Children’s Foundation, the substance use disorder (SUD) treatment center focuses its work on supporting youth and adolescents in the metro Detroit region.
For perspective, last year, approximately 53,000 12- to 17-year-olds in Michigan reported having a substance use disorder (MHA, 2023). The average cost of out-patient treatment is $5,000, and Michigan is ranked 5th worst in the nation with 4 million people living in areas that have a shortage of mental health professionals (NAMI,2023).
Simply put, our youth are struggling and the barriers to accessing care are many.
AARC supports kids who have fallen into difficulties with substance misuse and overuse that is impacting their lives. Their average patient’s age is 16, but AARC has treated kids as young as 12 and will accept youth for treatment until 18, regardless of insurance or ability to pay.
We recently sat down with AARC’s Matt LaCasse, D.O., and Marlene Joshi, MA, LPC, CAADC, who are providing patient treatment, to discuss that past year and what they want the community to know. Here is what they had to say:
1 – What are some reflections on the past year?
The year has gone really well. We are happy to be here, and it has been wonderful to grow AARC in reach and impact of so many kids.
Though kids are often forced to get treatment, they become willing participants. Once they realize AARC is a safe spot where they can talk about their challenges, kids generally dive in and want to stay.
We’ve encountered teens taking opioids and failing out of school, living between being high and withdrawal or managing conflict. Parents are traumatized and at their wits end; the school is threatening action. We’ve watched those kids work through their struggles and evolve into building relationships with their family and peers, getting good grades, and putting the effort into sobriety.
It’s not a straight line though; kids are week to week. If things in life are going well, they’re thriving; if they’re dealing with some sort of conflict, everything is more intense. But consistency is what we are looking for. Even if the kid is not necessarily doing well – they’re still choosing to come here. They’re still choosing to get help.
Certain cases are especially hard to hear about because they are reminders that young people really struggle with difficult things. They turn to substances as coping mechanisms, but we at AARC get to experience their resiliency and its commendable.
Over the course of the year, we’ve seen 61 patients and are seeing exponential growth month over month. That’s 61 kids who have their own experiences with sobriety. That’s 61 kids who will one day have families of their own. These kids will become adults who interact with their community, so learning how to healthily cope through life’s challenges now will have widespread impact for generations to come.
2 – How are patients finding AARC?
We are getting most of our patients via Michigan Department of Health and Human Services, Children, Youth & Family Services, as well as schools, court systems, and our rapport with hospitals in the area continues to grow. Hospitals are referring patients after short-term/acute hospitalizations seeking further help. Word of mouth amongst patients and families is becoming more common, too.
There is no other youth out-patient programming in our region like the one we offer here, so we are seeing how valuable a resource we are to the community. There are no referrals necessary to come visit us. Parents can call and we’ll do some triage and make sure kids are a good fit for the clinic and get them scheduled.
3 – What are some themes you are seeing?
Addiction pans all socioeconomic levels, all educational levels, all races and ethnicities. Kids who suffer through childhood with different issues are at an increased risk for SUD and mental health struggles, so we are treating kids from all walks of life.
We are providing psychotherapy to all patients. In addition to SUD treatment, some need other psychiatric care for depression, anxiety, trauma, PTSD, bipolar disorder, etc.
However, about half of our patients are experiencing pandemic related mental health issues and SUD. In other words, these kids developed challenges that stem from stress and isolation brought on by the pandemic. Although the pandemic might be over, it will have long-term effects and mental health and SUD are revealing themselves as common outcomes.
Kids have a hierarchy of substances; alcohol use has declined – marijuana and vaping have increased, which is what we are seeing the most; they are becoming an epidemic. Youth are developing physiological dependence to each of these, so much so that when they stop, they are anxious, they can’t see straight, they’re sweating, not eating, or sleeping.
Even though smoking cigarettes is not as common as it used to be, vapes contain nicotine, TCH, and many other toxic chemicals all harmful to one’s health. The general community’s perceived risk of marijuana has dropped significantly and that’s partly because of the legalization of it. Our patients are telling us that they have very few friends that don’t engage in the use of THC.
About 10% of our patients have misused opioids. Opioids are the most dangerous substance, though they all can lead to major troubles. This doesn’t mean that opioid use isn’t prevalent, it just means that kids are using THC and vaping more often than misusing pills.
4 – How are the families involved?
The work we do is treating the kid with the understanding that they live in the family unit. Our approach is for the kid to play a role in breaking barriers that have gone up because of their previous behaviors. This is routinely reinforced and addressed with patients. We have programming and capabilities to do family therapy as well, which does positively impact the patient’s progress and long-term recovery.
Getting full family participation is challenging, though. Parents are involved daily with their child’s care, but the thought of therapy is either scary for people or logistically challenging. We understand and continue to educate the community on the value of therapy because it is so beneficial to someone suffering with SUD to have their loved ones understand the disease and challenges of it.
5 – How do you transition cases or age-out kids?
We only discharge folks if we mutually agree they are doing well enough to not come back. There are some patients that have chosen to continue maintenance appointments once a month. Our clinic model is set up that we continue to monitor kids through young adult because relapses are common. Keeping them connected to the clinic is really important to us.
6 – Why is the philanthropic component of AARC so important?
Philanthropy allows us to care for the kids to the degree that we do. It makes it all possible.
We can spend two hours with a kid and that doesn’t happen in most other practices; psychiatrists typically squeezed in 15-minute sessions and that’s not enough time to provide comprehensive work to treat everything that’s going on with a kid.
We accept all patients regardless of their ability to pay. If the patient has insurance, we will bill it, but we continue to spend the amount of time the kid needs regardless of their plan’s eligible criteria. If a patient doesn’t have insurance, or can’t afford the deductible or copay, their services are covered by philanthropy.
We simply couldn’t provide comprehensive care to get these kids healthy and on the right track without philanthropy, and we are so thankful for our partnership with the Jamie Daniels Foundation and Children’s Foundation that allows us to do our work.
7 – What do you want to say to parents out there?
Kids explore new experiences, and sometimes that includes using substances. Have open communication with your kid. Even if you suspect there is no danger, have the conversation. Be an honest and a supportive ear. There’s no need to be afraid to ask your kids questions.
A lot of this comes down to education; people simply don’t know what treatment looks like or what it looks like for kids to have these struggles. Support your kids, know we are here as a resource, and be open to rebuilding your relationship with them.